{kind=link}
Saba is a cute orange cat, male, neutered, 8 years old.
The chief complaint was: non-healing wounds caused by recurrent injection-site sarcoma on the thigh.
First visit (2024.01.17)
At the end of October 2023, Saba underwent resection of a mass on the lateral side of his left thigh in another hospital, and the pathology report diagnosed it as fibrosarcoma.
The operation at that time was a small excision along the edge of the mass. The wound was licked open a week after the operation and did not heal after that.
Since then, the wound has been cared for with open wound management, and the wound has been completely unresponsive to any oral medications.
As the weeks passed, the ulcers in the wound became more and more serious, and the remaining tumor cells at the bottom of the skin quickly grew back, becoming more irregular than before.
The center of the tumor began to break, ulcerate, and rot. As a result, Saba had to endure severe pain. Everything he touched or the room he stayed in would emit a strong putrid smell.

Our discussions with parents in the clinic focus on three main points:
This diagnosis of fibrosarcoma is likely to be an injection site sarcoma in cats, so it must be considered more malignant than ordinary soft tissue sarcomas.
A normal post-surgical wound, no matter how serious the infection is, will not evolve into this over time. This is a typical tumor recurrence and requires a more radical surgery.
Can the tumor be cut completely? We can’t give an answer right now. We need to shave all the hair in this area, and debride the wound, and then demarcate the expected margin of surgery. Moreover, the cat is very aggressive, he must be sedated before the evaluation can be carried out.
Wound debridement and preoperative planning (2024.01.23)
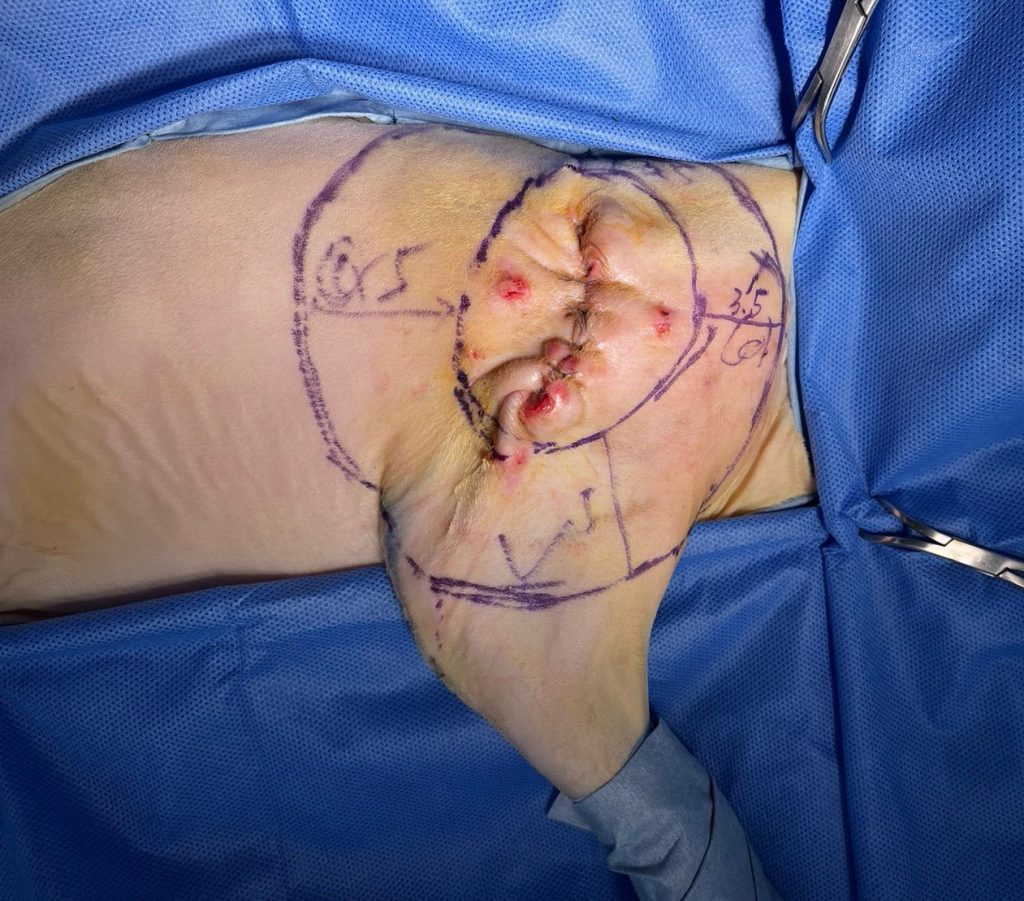
We sedated Saba, shaved the hair around the wound and the entire half of the abdominal wall, then clean and debrided it.
You can see after shaving that the recurrent tumor is located in the proximal 1/3 of the left thigh. It does not invade the pelvis or is close to the pelvis under X-ray.
When I first met Saba, I felt that the tumor was too large to be dissected. Fortunately, after shaving all the hair, I found that the area invaded by the tumor was not so desperate. Surgery was a reasonable and appropriate solution.


The first red circle we drew is a radius of 3 cm, and the second red circle is a radius of 2 cm. Because sarcoma at the injection site is a very malignant tumor, it must be removed with an lateral margin of 5 cm, so the second red circle is the margin we expect to resect.
From this point of view, this foot must be amputated, and a lot of muscles in the hip and back must be removed.
You can see that the red circle is actually very close to the cat’s penis and anus area. We hope not to damage these two structures because I don’t want the cat to have to endure the inconvenience of losing one foot and incontinence after the surgery. The pain of urinating and defecation incontinence is so great that we will make some compromises in these two areas. It doesn’t matter if the range of resection does not reach 5 cm.
Finally, we have to think about how to close the wound after resecting such a large area?
We considered using the skin on the abdomen and the inner left thigh for closing the defect. The skin in these two areas is loose, so it should be no problem.
Efforts before surgery
Since Saba has been dealing with such serious wounds for a long time, his white blood cells are very high, and there is a very high chance of bacterial infection deep in the wound. We decided to spend some time to adjust his physical condition before the operation and to protect the wound.
Although it is impossible to heal ulcers caused by tumors, it is still necessary to remove the decayed material as much as possible before surgery, and to ease the inflammatory reaction in the surgical area, so that the success rate of the surgery will be higher.
Use tie-over bandage to protect the wound, and frequently replace wet gauze to achieve mechanical debridement, hoping to remove all the slough before surgery.
The good news is that Saba’s appetite is quite stable. We prescribe antibiotics and anti-inflammatory analgesics to relieve the discomfort caused by the wound. During the operation, the entire hindlimb should not be in an inflamed state, which will be harmful to the postoperative wound.

Surgery (2024.02.01)
During the operation, we determined by palpation that the deepest of the tumor was on the surface of the femur and did not penetrate deeper, so we decided not to remove the pelvis.
First define the lateral margin, draw a circle with a radius of 5 cm with the tumor as the center. If it is very close to the penis, anus, and tail, the margin will shorten to 3.5 cm.
The tumor center still has a broken and rotten appearance. Although it is much better than when we first met, we still sew up the volcano-like wound first to prevent pus or bacteria from contaminating the surgical area during the operation.
Dissection of dorsal margin:
Cut all the way deep from the skin, through the thick fat until it arrives the fascia. Remove the entire superficial gluteal muscle and part of the middle gluteal muscle, and then dissect ventrally until the coxofemoral joint is exposed.
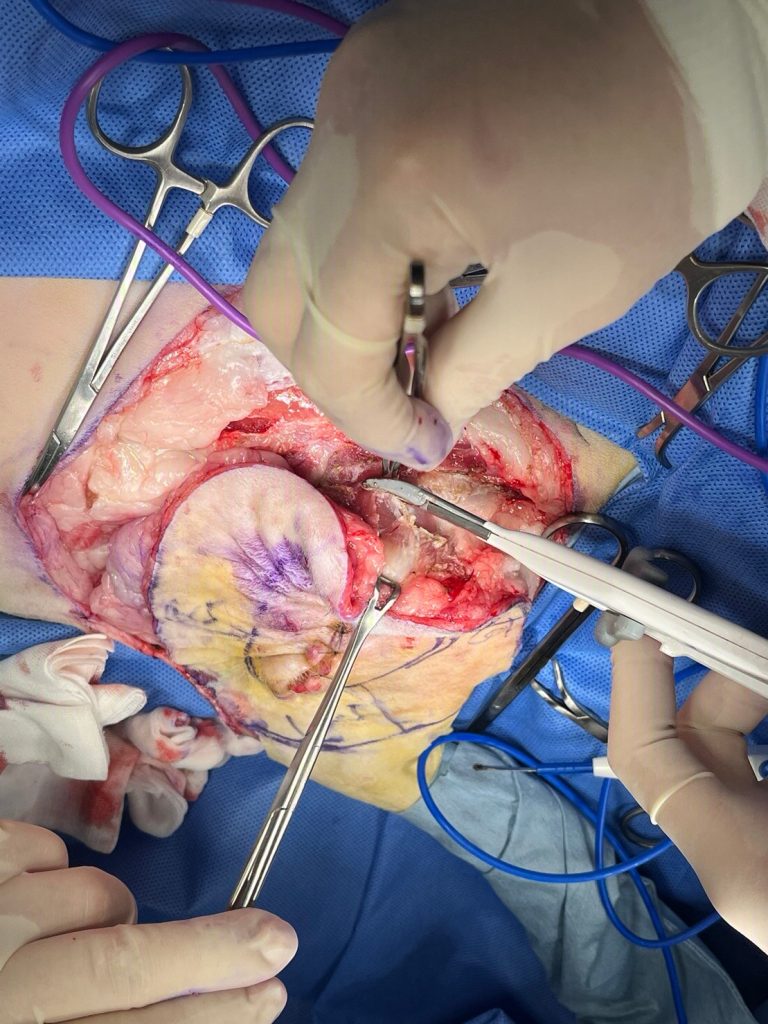
Dissection of cranial margin:
In the same way, cut deeply from the skin, then remove the external abdominal oblique muscle within the defined margin, and continue to cut posteriorly until the full thickness of the sartorius muscle cranial part is removed.
Dissection of caudal margin:
Because this region contains the tail, penis, and anus, the resection is more conservative. Remove the muscle 1 cm in front of the ischial tuberosity. Be very careful during the process and be sure not to injure the pudendal nerve, which is responsible for controlling defecation and urination.
Dissection of ventral margin:
This is the simplest part. The procedure is just like amputation of the hindlimb. We transect all the muscles 2 cm far from the inguinal fold. And ligate the femoral artery and vein.
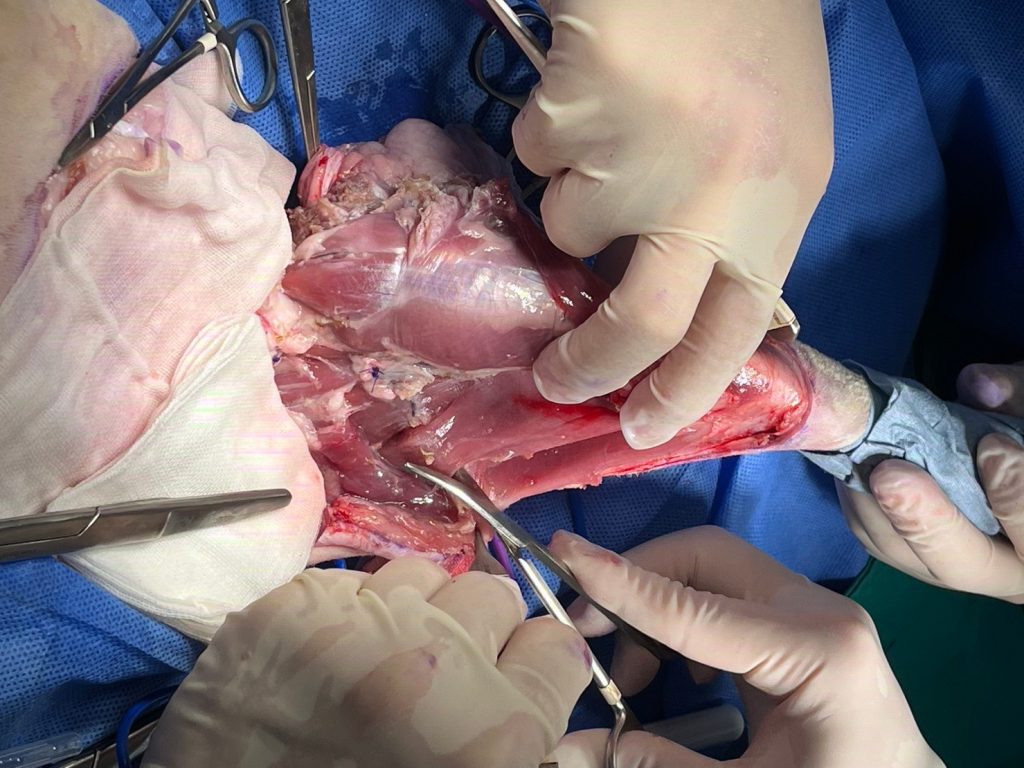
We left the skin, subcutaneous fat, and a small amount of remaining muscle connected to the inguinal fold on the inner thigh to help close the huge defect after tumor resection. At this point, the tumor and left hindlimb have been completely removed.
Close the defect:
Place the draining tube first.
Then the muscles are sutured, the subcutaneous fat is sutured, and finally the skin is closed, and the operation is completed.

Postoperative hospitalization (2024.02.01-03)
After such a major operation, hospitalization is necessary.
We continued to give Saba intravenous analgesics, changed the wound dressing every day, and also monitored his spirit and appetite.
Fortunately, the cat recovered very well. He was only weak the night after the operation (at that time, he even allowed me to touch his head gently). The next morning, he was back to the ferocious little tiger he was before.
After 2 days of hospitalization, because Saba’s spirit and appetite were stable, the wounds were stable, and the amount of fluid in the drainage ball was not much, we removed the draining tube and sent the cat home.
I thought everything would go smoothly from now on, but I didn’t expect…
Postoperative follow-up (2024.02.07)
Today is mainly to confirm the condition of the wound. This day is also the last working day before the Lunar New Year. The whole hospital is filled with an atmosphere of an upcoming holiday. We will not perform major operations or admit patients to the hospital on this day.
When I met Saba, he was still very fierce, so fierce that it was difficult to take him out of the cage.
The owners said that his appetite has been about half of its original value in the past few days, his spirit is average.
The cat had normal defecation every day, did not vomit, and was given oral medication.
As for the wound, the owners said that it was fine under observation at home, but there was some exudation in the past two days, and occasionally a small amount of fluid leaked out from between the sutures.
In fact, it sounds like this is an acceptable behavior for a cat that has just undergone major surgery, but since it is the Lunar New Year holiday, I definitely have to check it out carefully. If I let the cat go home carelessly, we will not be able to track the wound status for 7 days.
So no matter how many outpatient visits waiting outside the room, we still patiently take the cat out of the cage and onto the treatment table.

When I measured the cat’s weight, I found he had lost half a kilogram, and he still had a putrid smell. The parents said that the smell may be due to the catmint not being cleaned, because this catmint was used every time when going to the hospital.
It was quite reasonable. After all, we were doing the surgery ourselves, and I was confident in the sterile operation during the surgery. “The smell should come from the cage, not the cat,” I thought to myself.
I started to check the wound area by area, and found that the skin in the back part of the wound was swollen. Pressing could indeed squeeze out the secretions, and the secretions were a bit pus-like. It was still difficult for me to confirm whether the secretions were smelly, because The entire cat, and even the entire clinic, was filled with a putrid smell.
From my experience, this kind of discharge is not normal.
I decided to put the indwelling catheter on the cat and prepare to confirm the wound condition after sedation in the afternoon. The wound may need to be opened and debrided.
I also did a blood test for the cat. Originally, I had no special expectations about the blood test results, but the results made me very worried. Neutrophil 980 (normal range 2300-10290), monocyte 10160 (normal range 50-670), one is very low, and the other very high, combined with other indexes and a very high body temperature, the cat may have a wound infection or even sepsis.
I started not to be careless about the sedation and debridement in the afternoon.
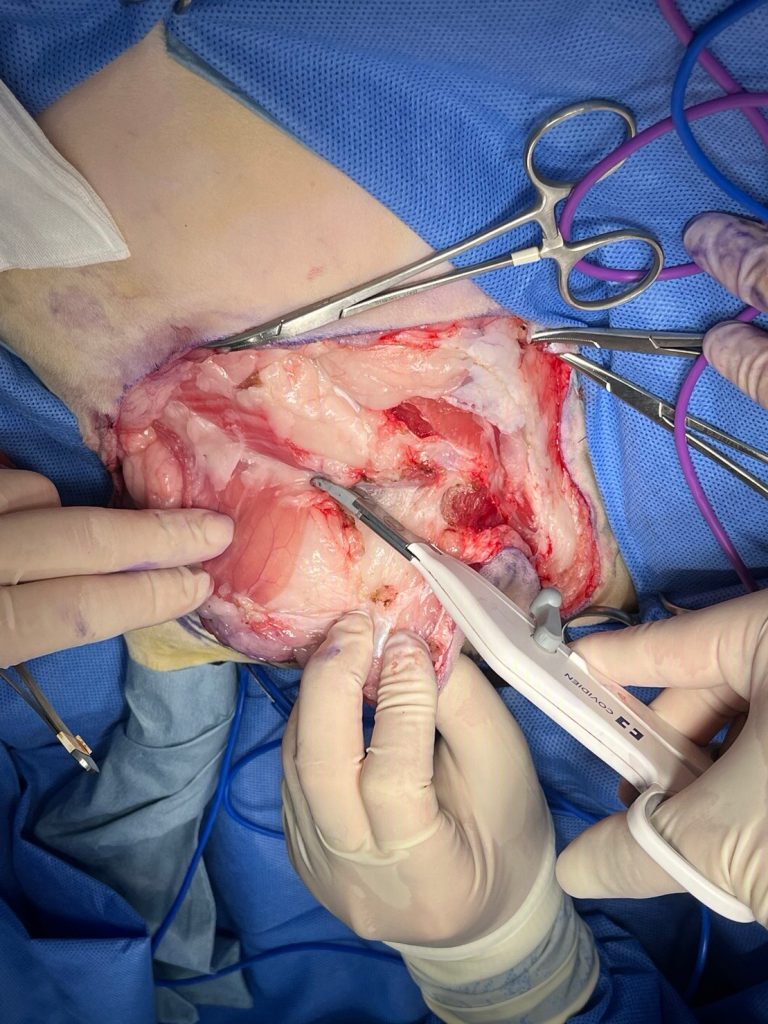
Debridement surgery
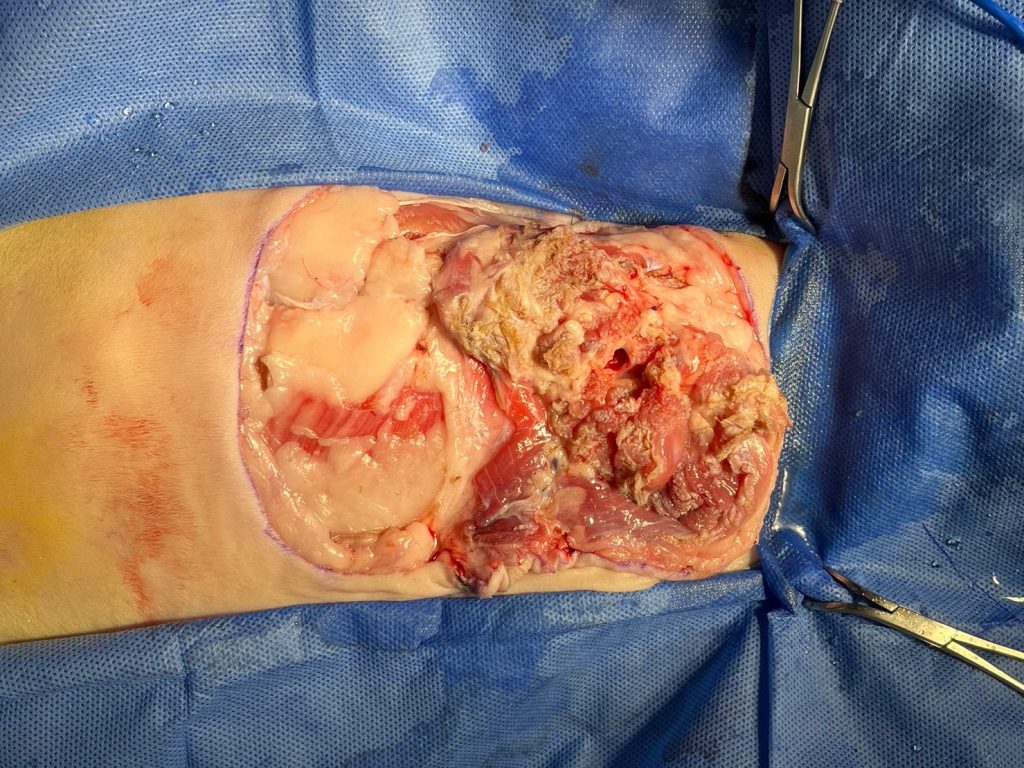
After cutting the original sutures of the wound, it was found that a large amount of foul-smelling pus-like fluid gushed out, and many parts of the muscle layer and subcutaneous fat layer were also in a state of necrosis and decay.
It turned out that the putrid smell on the cat in the morning did not come from the unwashed catmint, but was really the smell of wound exudate.
This is definitely bad news.

First, remove the necrotic muscle and subcutaneous fat layer as much as possible, and then trim the necrotic skin. This action will make it difficult to close the wound smoothly (because during the first operation, the tension between the skin and the skin is very high). However, if the necrotic area is not completely removed, it may leave a source of infection, so it still needs to be done.
For the necrotic and rotten flesh, I trimmed it with scissors and rubbed it back and forth with my fingers, hoping to remove it cleanly.
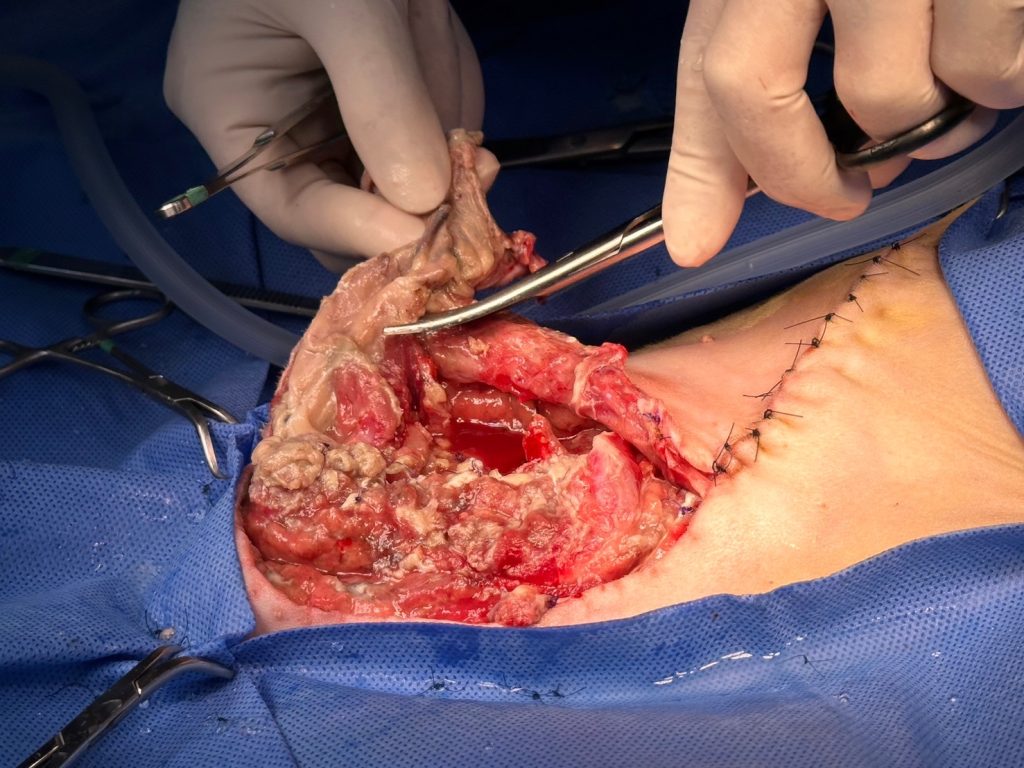
We treat the wounds in one area and one area at a time, while irrigating with a large amount of sterile saline water, and try to treat the entire wound to a relatively clean level.
After the cleaning, the putrid smell in the air was no longer so strong.
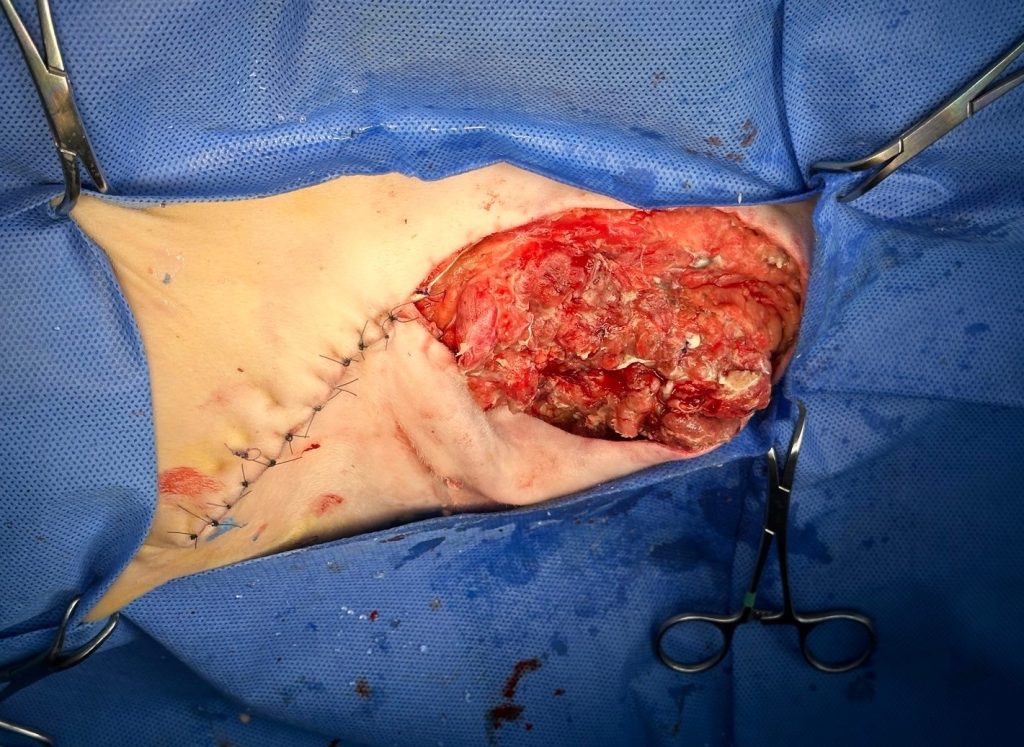
Because I was not sure whether there was any remaining source of infection, sewing the wound back up at this time would undoubtedly give the remaining bacteria a chance to thrive again. So we decided not to close the wound and sewed the skin to the muscle, creating an open wound 15 cms long and 3 cms wide.
Cause of infection
I think it may be because of the original rotten wound. Even if we start taking care of it a few days before the operation, and give antibiotics to the cat in advance; even if the wound surface is closed and then scrubbed during the operation, there may still be some sources of pollution quietly hiding in it. surgical area, causing postoperative bacteria to re-grow in fresh, fragile wounds.
No matter what, you have to face it when it happens.
After the operation, the cat will remain open and apply honey and gauze every day. It is still unknown whether the cat’s body can survive the septicemia.
Successive hospitalizations
Because our hospital will be closed for 5 days starting from the next day, after discussing with the owner, we transferred Saba to a trustworthy 24-hour animal hospital for continued treatment. They are open during the Chinese New Year.
Saba was transferred to the hospital that night and started a series of hospitalization monitoring, including intravenous infusion, antibiotics and analgesics, monitoring of appetite and physiological values, changing bandages and cleaning wounds once a day.
This vacation was really difficult for me. I thought about this cat vaguely every day. Fortunately, the doctors at the animal hospital were very careful and would send me messages every day to inform me of the cat’s physical condition and wound status.
The open wound is slowly improving with daily debridement and dressing.

A week later, as the wound gradually stabilized, the cat’s condition also gradually recovered.
Secondary debridement and wound closure (2024.02.17)
It has been 10 days since the debridement before the Lunar New Year holiday.
The cat finally returned to our clinic.
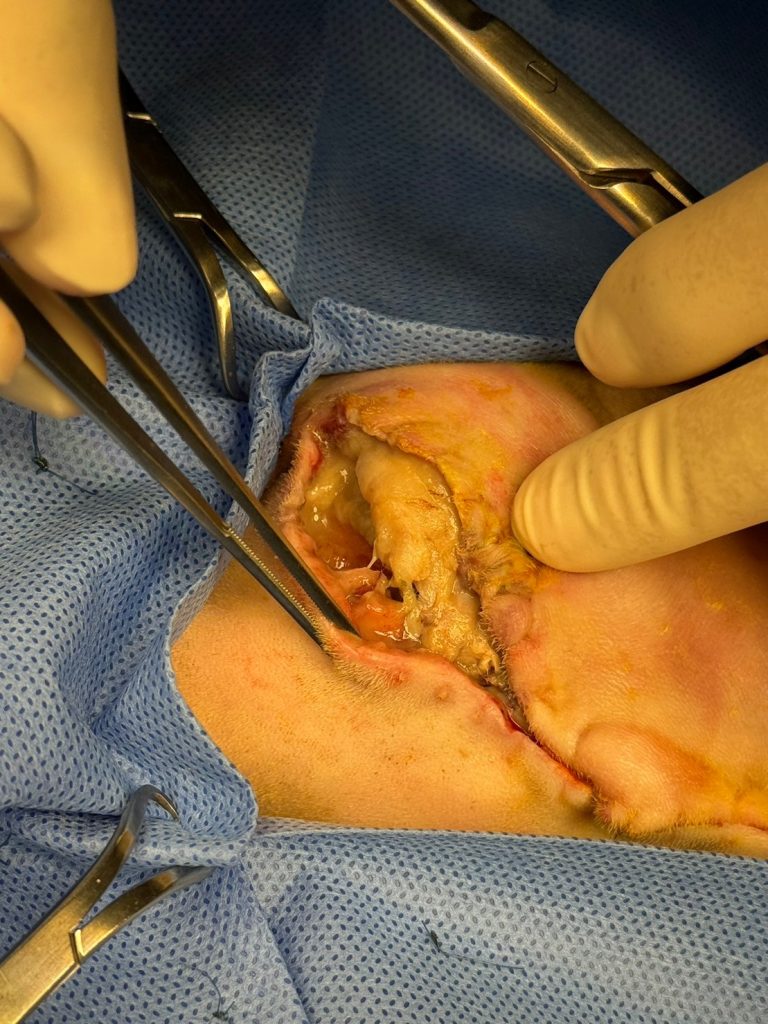
His energy and appetite were normal, but the back of the wound was still a little bulging, so I had to arrange another debridement surgery for him in the afternoon.
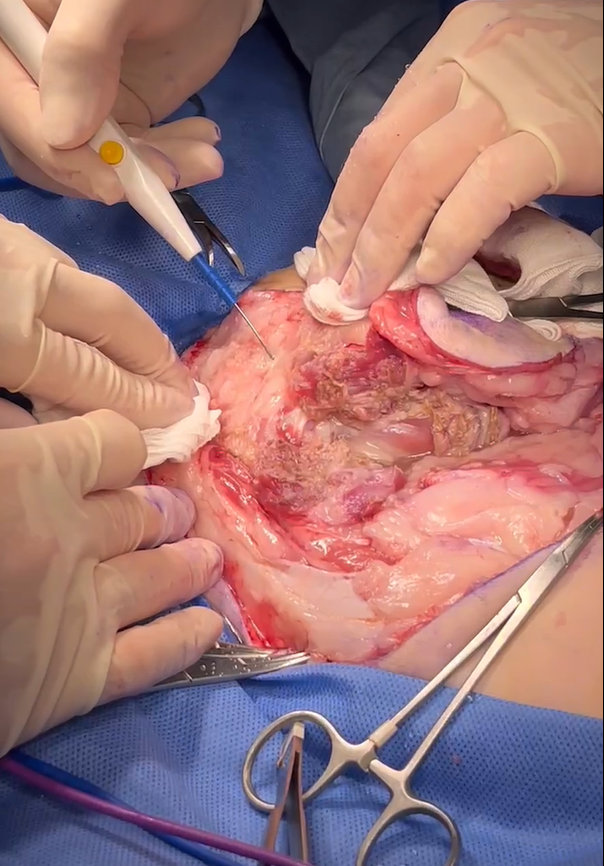
During the operation, we found a space on the dorsal side of the open wound (that is, the cat’s dorsal side) hiding a large amount of pus. We cut the upper skin to allow the pus to drain out.
The pus this time was no longer as smelly as the first debridement, and I couldn’t even smell it after smelling it carefully, which made me feel a little relieved.
I deliberately left this incision open and treated it as an open wound.
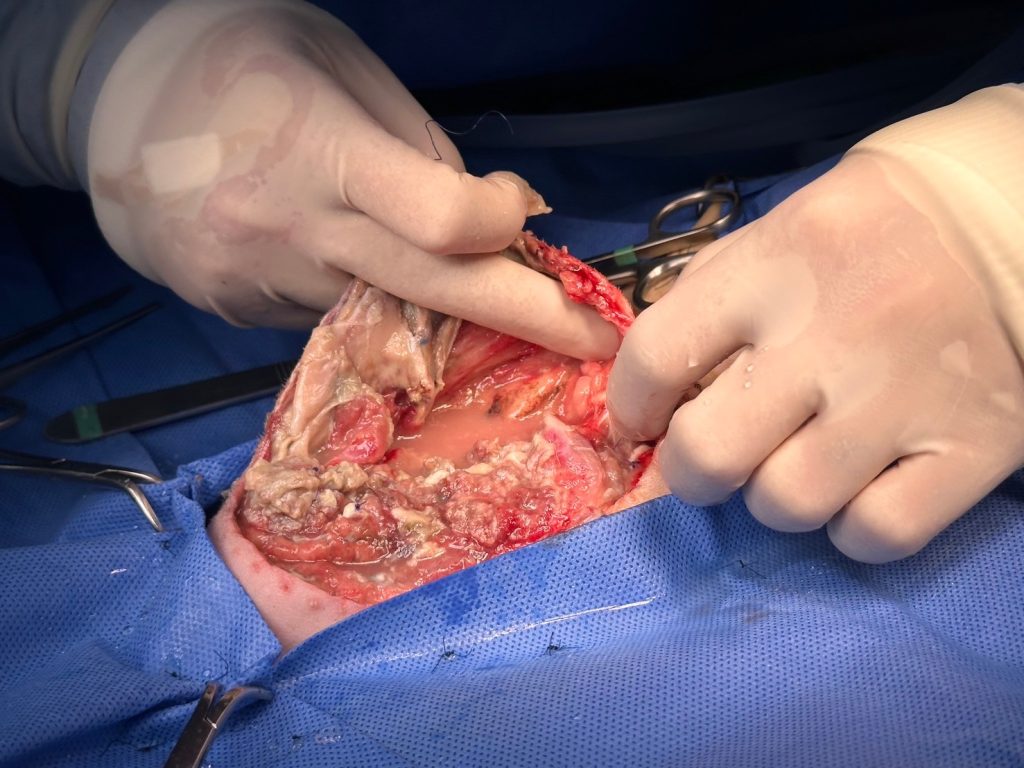
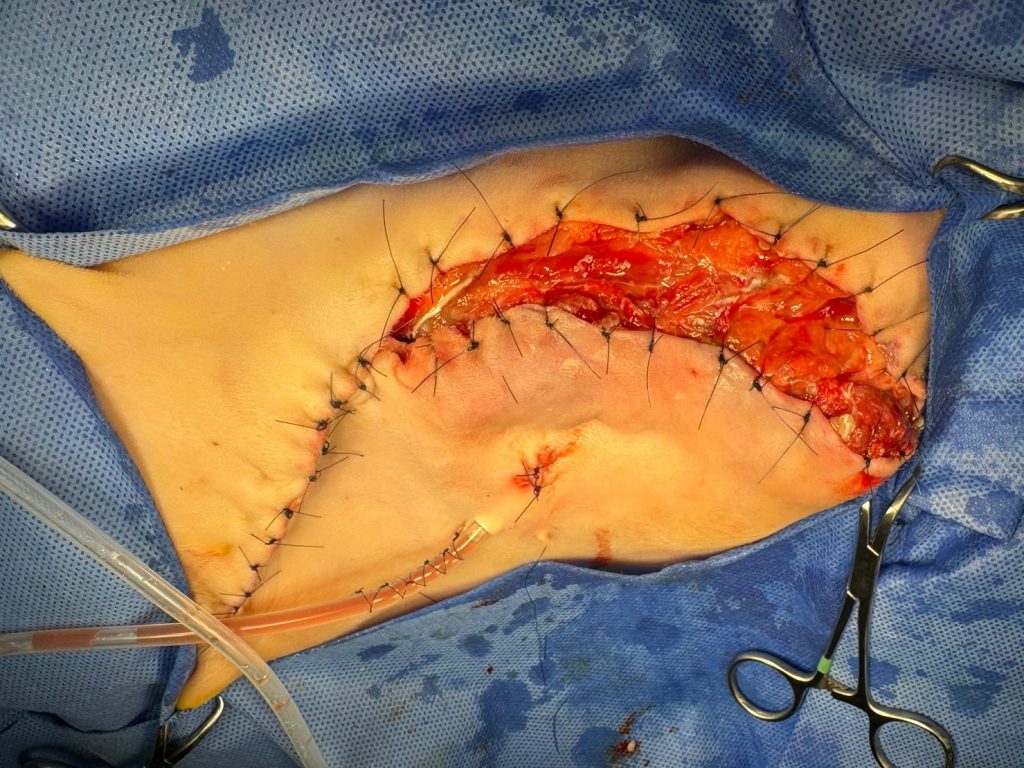
In the wound area that was originally open, red and healthy granulation tissue has grown very thick, which means that the wound has been eliminated from infection. We separate it from the skin and scrape off a certain thickness of granulation tissue so that the skin on both sides can be aligned.
This very large open wound, which took care of for 10 days, was finally closed by us.

Pathology report
The diagnosis was malignant fibrosarcoma, and the surgical margins were all clean with no residual tumor.
It’s great that the popliteal lymph nodes have not been metastasized.
There is no obvious evidence that the tumor is an injection site sarcoma. However, based on the cat’s age, medical history, and location, it is definitely safer for the cat to treat it as an injection site sarcoma.

Days of recovery (2024.03.02)
After so much torture, Saba’s wounds could finally have their stitches removed.
Seeing that the wound was healing well and the cat was regaining its former vitality, I finally felt relieved.


Discussion
Injection site sarcoma in cats is highly invasive locally and has a high recurrence rate. It is a tumor that must be extensively removed. I saw some people on the Internet saying that “injection site sarcoma will definitely recur after surgery, so you must not do surgery.” I think this is unfair to the cats.
Studies have proven that with good surgery and extensive resection (lateral margin 5 cm, bottom two layers of muscle membrane), the median survival time can reach 901 days, the local recurrence rate is 14%, and the metastasis rate is 20%. Although the recurrence and metastasis rates are still high, they are definitely not that desperate.
There is only one key point: “early detection”. If parents discover the tumors when they are smaller, the success rate of large-scale surgical resection will be improved, and the recurrence and metastasis rates after surgery will be reduced.
After surgery, it is important to make appointments with parents for regular follow-up visits to confirm the status of wound recovery. And during the consultation process, don’t miss any detail, no matter how ferocious the cat is.
When encountering complications such as postoperative infection, necrosis, and suppuration, we must face them bravely as soon as possible. Only in this way can we gain a chance of survival for our patients.